


Limited reproductive health care options harm Rockbridge County residents
W&L faculty share their experiences with high-risk pregnancies and off-road deliveries
May 8, 2023
Jodi Williams was 15 minutes away from the hospital when she realized she wasn’t going to make it in time to give birth.
Her husband pulled the car over onto the highway shoulder and jumped out. Two minutes later, they were back on the road, a newborn baby girl in Williams’ arms.
Williams never imagined this would be part of her experience.
“The scary part is, you think you’re going to make it, and there was definitely no way to make it to the hospital,” said Williams, who is the executive director of human resources at Washington and Lee University.
Since the labor and delivery unit at Carilion Rockbridge Community Hospital closed in 2010, women in Rockbridge County have to travel nearly an hour to deliver their babies.
Some advocates have described Rockbridge County as a health care desert because of the lack of quality health care options. There is no labor and delivery unit, neonatal intensive care unit, fertility care, or even OB-GYN care offered on a daily basis within county lines.
Without adequate access to reproductive care, Rockbridge County is a rare example of an area unaffected by the June 2022 overturning of Roe v. Wade. A woman’s ability to have an abortion in the rural county remains restricted.
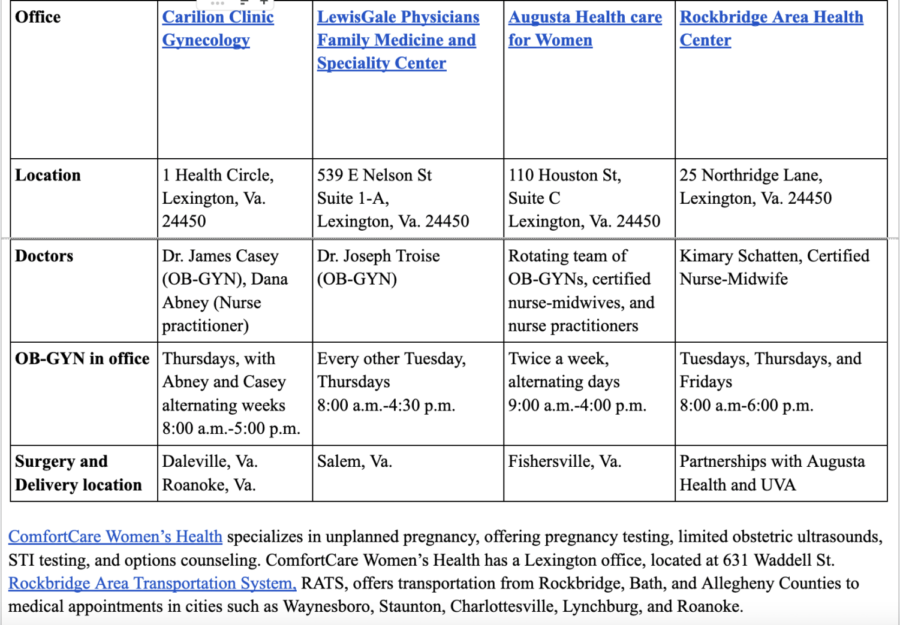
Augusta Health Care for Women, Carilion Clinic, and LewisGale Physicians offer gynecological care in Lexington one to two days a week, with main offices and hospitals outside of Rockbridge County. At these offices, appointments include breast exams, IUD insertions, biopsies, general visits, labs and labor checks.
The closest hospital for delivery is an Augusta Health office located in Fishersville, a 40-minute drive away. For fertility care, high-risk specialists, or neonatal care, patients have to drive an hour to Charlottesville or Roanoke.
Kimary Schatten provides gynecological services at Rockbridge Area Health Center (RAHC), a community clinic that provides services to patients regardless of their ability to pay. RAHC is the only organization in Rockbridge County that qualifies for federal funds under Title 10, which supports free and reduced-priced birth control.
Even though RAHC has the time and resources, Schatten said cultural perceptions keep many patients from coming in. While 200 people have babies every month in the county, Schatten said she only provides care for about 10 deliveries a month.
With the increasing privatization of health care systems across the country, Carliss Chatman, an associate law professor at Washington and Lee, said that wealth and power determine where hospitals are located — not need. According to the U.S. Census, Rockbridge County has 22,593 residents spread across 597 square miles. With such a low population density, Rockbridge County is not the most profitable place to build a state-of-the-art facility.
Living in a health care desert affects residents in different ways, Chatman said. The effects are especially acute for marginalized groups, including those without reliable transportation or the time to drive two hours round-trip.
“What about the women who are working minimum wage jobs, who have childcare issues, and other issues– what happens when they need health care?” Chatman said. “The lack of labor and delivery is a sign, for me, that all things are lacking.”
Rockbridge Area Transportation, RATS, provides medical transportation to nearby counties, but patients have to schedule their rides in advance.
Carilion Rockbridge Community Hospital, then named Stonewall Jackson Hospital, closed its labor and delivery unit in April 2010. In a news release, Dr. Thomas McNamara, hospital president, cited supply and demand decreases as the reasons for closure.
“We held on as long as we could,” McNamara said. “We simply don’t have enough patients and physician participation to continue.”
Marisa Charley, director of the service-oriented Bonner Program at Washington and Lee, thinks reopening a labor and delivery unit at Carilion is not the answer.
“I think there are a lot of reasons that the hospital in Lexington would not be an adequate space, even if there was another provider,” Charley said. “I think that there are important questions that are being asked about quality of resources and quality of care that are available in rural spaces.”
Charley experienced two high-risk pregnancies. For her second, Charley used IVF to conceive, which forced her to drive to Charlottesville three days a week for blood draws and ultrasounds — and make it back to Lexington by 9 a.m. for work.
“When I had bleeding early in my pregnancy, there was nobody in the city of Lexington who could give me an internal ultrasound that could have told me if I was losing my baby or not,” Charley said. “That’s not OK.”

Charley had two medically necessary abortions: one for an ectopic pregnancy and one for an incomplete miscarriage. If left untreated, both can be fatal.
“What happens when you don’t get an abortion?” Charley said. “You die.”
It’s these types of situations that inspire advocates like Washington and Lee English professor Brenna Womer.
The day she heard about the Roe v. Wade decision, Womer immediately decided to protest.
“I didn’t shower or anything. I can’t remember if I brushed my teeth,” Womer said.
For the next three weeks, Womer went to the corner of Nelson and Main Street with a freshly painted sign.
Womer was overwhelmed by the community response. Drivers honked their horns; children asked questions. Some even joined her protest, staying for five minutes or two hours.
Womer said her goal was to be a constant presence in a time of uncertainty.
“There is so much stigma and shame attached to and associated with abortion,” Womer said. “If they have all these forces in their life that are saying, ‘If you have an abortion, you are committing murder,’ I hope that my sign will pop into their head. Abortion is OK. It is essential. It is sacred.”
According to Schatten, these hardwired beliefs against abortion permeate the way people access reproductive health. She said that most of her patients won’t consider abortion, even if they are in unstable or dangerous situations without housing, income or partnership.
“I think it just goes back to a cultural, religious, southern, conservative environment where that has just been really ingrained in young girls that that’s just not an option,” Schatten said. “You don’t do that. If you ‘mess up’ and get pregnant, then you have to deal with it and have a baby.”
On top of these expectations, Chatman said that between proposed bans and legislation in other states, many women don’t even know that abortion is currently legal in Virginia. This lack of information and knowledge serves as a “ghost ban.”
“If you think you don’t have access to reproductive rights, it’s the same as not having access, because you’re not going to try,” Chatman said.
Schatten said that it is hard to be a provider in an area where cultural beliefs and lack of resources work against access to reproductive health services.
“All we can do is make little drops in the bucket along the way and hope it’s affecting one person at a time. You know it’s really easy to lose hope,” Schatten said. “But every time I put in an IUD and I’m like, ‘Oh, someone’s not going to have an unplanned pregnancy for at least five to eight years,’ I’m very, very pleased.”
Michael McLaughlin '23 • Sep 21, 2023 at 9:54 pm
It is a shame that there isn’t any true reproductive health care available in Rockbridge County. And by true reproductive health care, I mean the kind of care that ensures the help of healthy reproduction, not the killing or preventing of the next generation. It is also a shame that Rockbridge County has not advanced in reproductive health after the overturning of Roe v. Wade. All of the governmental money being used on abortions should instead be funneled into ensuring that each mother has a healthy delivery of her baby, and not in an outlandish location. If this requires traveling doctors and nurses like in the days of old should a delivery clinic not be built, so be it.
To the “cultural, religious, southern, conservative environment” that we are in: I am proud of you. I would not have it any other way. I am glad that the people of Rockbridge County show disdain toward the murdering of babies, and I am glad that they instill the value of responsibility in their children that when they ‘mess up,’ they face the consequences. There is only one natural cause for a child, and one natural effect. And the best way to obtain this knowledge is from the natural, rural environment surrounding us, where we can learn from the animals in the farms as they go about their natural animal lives.
Finally, abortion is certainly NOT sacred. The only person for whom abortion is sacred is Satan. No holy being requires or approves of the sacrifice of children. This is true for every major religion, everywhere. Only evil encourages such behavior. I pray that Ms. Womer stops misleading young women into the killing of their children, and I ask that the protesters cease their taking advantage of people with mental disabilities for their own optics, especially as they celebrate the aborting of the many disabled children who are killed simply because of their own existence.
Anonymous Elephant • May 10, 2023 at 2:52 pm
I feel bad for Brenna Womer